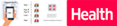
The lungs are the center of the respiratory (breathing) system.
Every cell of the body needs oxygen to stay alive and healthy. Your body also needs to get rid of carbon dioxide. This gas is a waste product that is made by the cells during their normal, everyday functions. Your lungs are specially designed to exchange these gases every time you breathe in and out.
Lung Cancer
Cancer is a disease that begins at the cellular level. The cells are the building blocks of all the tissue in the body, and in their healthy state, they grow and divide as the body needs them to maintain the current structure. As cells get old or become damaged, they die, and new cells replace them. Cancer develops when the cells become abnormal, reproduce at high rates, and create tumors. Cancerous tumors can also invade surrounding tissues and may spread to other areas of the body.
Lung cancer is a type of cancer that begins in the lungs, the main organs of the respiratory system. Lung cancer is the leading cause of cancer death and the second most diagnosed cancer in both men and women in the United States. Lung cancer claims more lives each year than do colon, prostate, ovarian and breast cancers combined.
Most lung cancers are carcinomas – cancers that start in the cells that line the inner and outer surfaces of the body. Lung cancers are categorized as small cell lung cancer or non-small cell lung cancer, named for their appearance under a microscope. These different types of lung cancer grow and develop differently and are treated differently. The most common is non-small cell lung cancer.
Small Cell Lung Cancer(SCLC) is the minor type (15%) that spreads quickly from the lungs to other parts of the body. Non-Small Cell Lung Cancer (NSCLC) is the most common type (85%) of lung cancer.; subtypes are Squamous cell carcinoma, adenocarcinoma, and large cell carcinoma
Primary treatment: (a) Chemotherapy alone, (b) Chemotherapy together with Radiation. Which way to go? Doctor decides based on the stage and situation of the disease
Limited-stage case: (a) tumor present in only one -may spread to nearby tissues but not spread to other regions of the body = combination of chemotherapy and radiation therapy
Extensive-stage case: tumor already spread to other parts of the body = chemotherapy only (some cases, radiation therapy is used to improve symptoms or to prevent the cancer from spreading to the brain)
Initial chemotherapy after diagnosis: combination of the drug etoposide with either cisplatin or carboplatin.
* Treat with Chemo Before Surgery (also called Neoadjuvant Chemotherapy)
The first place where cancer cells spread from the lungs is often the lymph nodes (also called lymph glands). This is because the lymph nodes act as a filter, trapping cancer cells as they travel out of the lungs. In this case, giving chemo for several months before surgery can improve the cure rate for NSCLC. For stage III cases, the cure rate can double. New drugs from clincial trials can be use for Neoadjuvant chemotherapy. (show example videos)
* Treat with Chemo After Surgery (also called Adjuvant Chemotherapy)
Your doctor recommends this treatment and the decision depends on the size of your tumor and often when lung cancer cells have spread to the lymph nodes. This appproach is more traditional approach.
Clinical Trials and New Drugs
* Treatments can be a new drug alone or in combination with more established drug treatments.
Cancer Stem Cell Therapy: Killing cancer stem cells to block rise of new type of lung cancer cells (show example videos)
IImmunotherapy: Drugs to stimulate patients’ own immune systems to recognize and attack lung cancer cells (show example videos)
Drug for Immunotherapy
Drug that block PD-1/PD-L1 pathway
Atezolizumab (Tecentriq®): approved for subsets of patients with advanced non-small cell lung cancer (NSCLC), including as a first-line therapy
Durvalumab (Imfinzi™): approved for subsets of patients with advanced non-small cell lung cancer (NSCLC)
Nivolumab (Opdivo®): approved for subsets of patients with advanced non-small cell lung cancer (NSCLC) as well as those with metastatic small cell lung cancer (SCLC) that has advanced following treatment with platinum-based chemotherapy and at least one other line of treatment
Pembrolizumab (Keytruda®): approved for subsets of patients with advanced non-small cell lung cancer (NSCLC), including as a first-line therapy
Targeted Therapy: Drugs target specific marker on lung cancer cells. Doctors will look for cell shape and appearance, genetic mutations and/or molecular targets (show example videos)
Targeted Therapy
Even tumors on original site are completely removed during surgery or destroyed by radiation therapy, some cancer cells nearby can still survive and start to spread again. New drugs from clinical trials may help to kill these lung cancer cells. (show example videos)
Radiation Therapy
External beam radiation therapy (EBRT) delivers high doses of radiation to lung cancer cells from outside the body, using a variety of machine-based technologies.
High-dose rate (HDR) brachytherapy (internal radiation) delivers high doses of radiation from implants placed close to, or inside, the tumor(s) in the body.
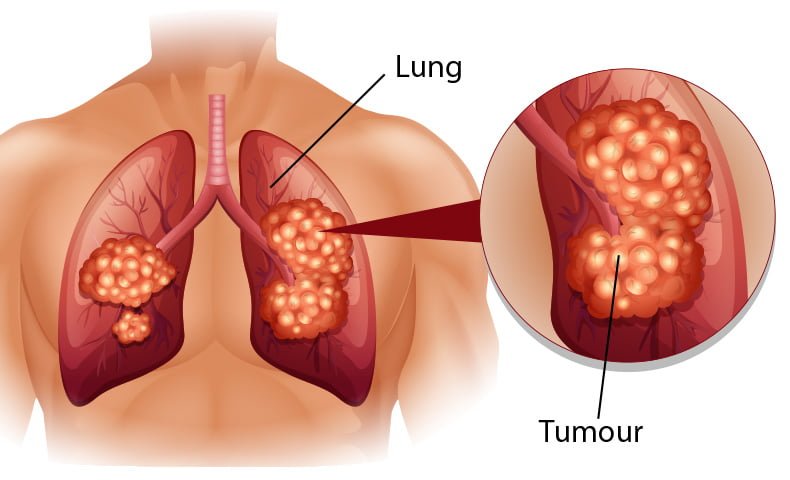
Smoking is the number one risk factor for lung cancer and thought to be responsible for 80% - 90% of all lung cancer diagnoses.
Using other tobacco products such as cigars or pipes also increases the risk of lung cancer. Tobacco smoke is a toxic mix of more than 7,000 chemicals are poisons.
Second-Hand Smoke
Smoke from other people’s cigarettes, pipes, or cigars also causes lung cancer. When a person breathes in secondhand smoke, it is like he or she is smoking. In the United States, two out of five adults who don’t smoke and half of the children are exposed to secondhand smoke, and about 7,300 people who never smoked die from lung cancer due to secondhand smoke every year.
Radon Gas
What is radon?
Radon is a radioactive gas released from rocks and soil. It is an invisible, odorless, tasteless gas that seeps up through the ground and diffuses into the air. Radon gas usually exists at very low levels outdoors and nearly all air. However, in areas without adequate ventilation, such as underground mines, radon can accumulate to levels that substantially increase the risk of lung cancer.
How does radon cause cancer and how many people exposure to radon?
Radon decays quickly, giving off tiny radioactive particles. When inhaled, these radioactive particles can damage the cells that line the lung. Long-term exposure to radon can lead to lung cancer, only cancer has proven to be associated with inhaling radon. Scientists estimate that 15,000 to 22,000 lung cancer deaths in the United States each year are related to radon.
More common in workplaces such as mines, mills, and shipyards, exposure to large amounts of asbestos puts you at a greater risk of developing mesothelioma, a type of cancer that starts in the lining surrounding the lungs. Make sure you use all protective equipment provided by your employer and follow all recommended safety procedures. If you are still concerned, see your doctor and/or visit the Occupational Safety and Health Administration website for more information.
Arsenic is a naturally occurring substance that can be found in air, water, and soil. It can also be released into the environment by certain agricultural and industrial processes, such as mining and metal smelting. Arsenic comes in two forms (organic and inorganic); the inorganic form is more toxic than the organic form.
People in the general population may be exposed to arsenic by smoking tobacco, being around tobacco smoke, drinking contaminated water, or eating food from plants that were irrigated with contaminated water. Inorganic arsenic is naturally present at high levels in the groundwater of certain countries, including the United States. Exposure to arsenic in contaminated drinking water is generally thought to be more harmful to human health than exposure to arsenic in contaminated foods.
Air Pollution
Air pollution is the harmful things that are found in the air we breathe.
It is a mixture of many different substances and the exact contents vary depending on its source, your location, the time of year and even the weather. Air pollution can be man-made, such as fumes from cars and smoke from burning fuels like wood or coal. But it also includes natural substances, like desert dust.
Previous Diagnosis or Family History
If you have had lung cancer, you have a higher risk of developing another lung cancer. Siblings and children of those who have had lung cancer also run a slightly higher risk of lung cancer themselves.
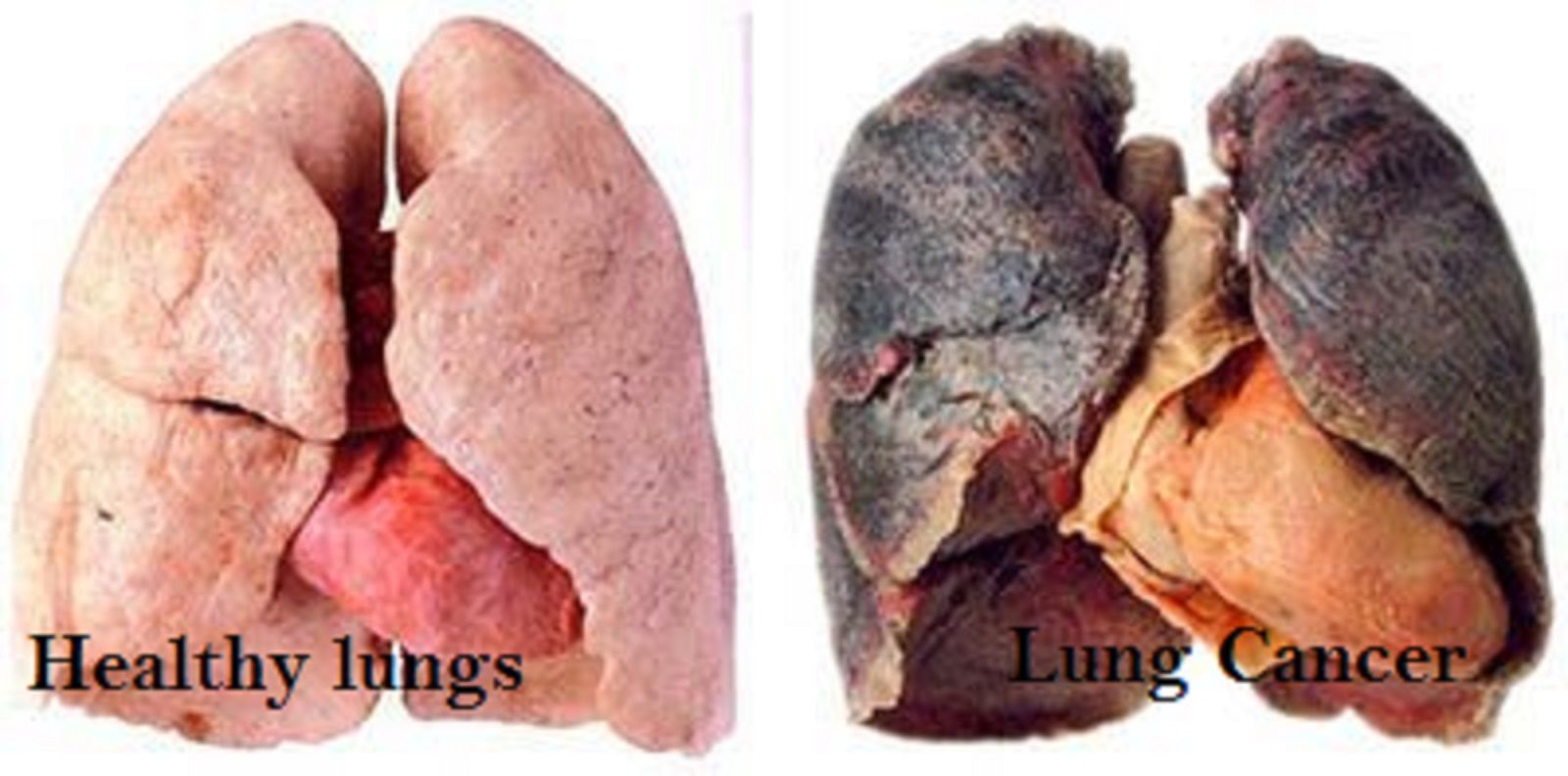
Most lung cancers do not cause any symptoms until they have spread, but some people with early lung cancer do have symptoms. If you go to your doctor when you first notice symptoms, your cancer might be diagnosed at an earlier stage, when treatment is more likely to be effective.
A cough that does not go away or gets worse (Constant coughing )
A cough related to the cool or respiratory disease will leave in up to 14 days; however, a constant cough that doesn’t end can be an indication of lung cancer.
Breathing difficulties (Dyspnea )
Difficult or uncomfortable breathing or a feeling of not getting enough air. 55-90% of lung cancer patients experience shortness of breath.
Coughing up blood (Hemoptysis )
The presence of blood in the sputum (spit or phlegm) coughed up from the lungs.
Hoarseness (abnormal voice changes)
Chest pain
Weight loss and loss of appetite
Feeling tired or weak
Recurring infections (Chronic bronchitis)
Others
Bone pain (spread to the back or hips)
Headache, weakness or numbness of an arm or leg, dizziness, balance problems, or seizures (spread to the brain or spinal cord)
Yellowing of the skin and eyes (jaundice) (spread to the liver)
Lumps near the surface of the body, due to cancer spreading to the skin or to lymph nodes (collections of immune system cells), such as those in the neck or above the collarbone
Non-small cell lung cancer is the most common type of lung cancer. Approximately 85% of all lung cancers are NSCLC. NSCLC occurs when malignant (cancer) cells form in the tissues of the lung. The major risk factor for developing NSCLC is smoking.
NSCLC has several sub-types, classified by the types of cells. Each type grows and spreads in different ways. The classification is determined by looking at the cancer cells under a microscope and is important because classification helps doctors choose appropriate treatment regimens, as well as determine the prognosis or projected outcome of the cancer .
Adenocarcinoma
Adenocarcinoma is the most common NSCLC (35-40% of all lung cancers) and usually occurs in a peripheral location within the lung, sometimes at the site of pre-existing scars, wounds, or inflammation. Adenocarcinomas begin in the cells that line the alveoli, the air sacs in the lungs that are responsible for the gas exchange of oxygen and carbon dioxide between the lungs and the blood.1,2 Additional characteristics of adenocarcinomas further describe the pattern of the cells under the microscope:
Acinar refers to cells in the shape of the alveoli.3
Papillary refers to the structure of the growth.2
Bronchioloalveolar is a subset of adenocarcinoma that arises in the outer bronchioles or alveoli of the lung.2,3
Mucinous refers to the tumor’s ability to create mucin, the main component of mucus.3
Squamous Cell Carcinoma
Squamous cell carcinoma accounts for 25-30% of all lung cancers and is found in the central parts of the lung, such as the bronchi. Squamous cells are flat cells that are found in the lining of the airways.2,4 Squamous cell carcinomas can be further described as papillary, clear cell, small cell, or basaloid, which refer to their appearance under the microscope.1
Large Cell Carcinoma
Large cell carcinoma accounts for 10-15% of all lung cancers and appears on chest x-rays as a large peripheral mass (mass in the outer regions of the lung). Under the microscope, cells of large cell carcinomas do not look like squamous cell carcinomas or adenocarcinomas. These tumors usually have a better prognosis than SCLC and are generally treated similarly to adenocarcinomas.2,4
Other Less Common Types of NSCLC
There are several additional, rare types of NSCLC, including:
Adenosquamous carcinoma, which refers to a cellular structure that is partly glandular (like adenocarcinomas) and partly surface cells (like squamous cell carcinomas)
Sarcomatoid carcinoma, which resembles a mixture of carcinomas that line the lungs and sarcomas (a different form of cancer) that arise from connective or supportive tissue
Pleomorphic, a subtype of sarcomatoid that is noted for having many shapes
Salivary gland carcinoma, which is named for its similarity to tumors which begin in the salivary glands
Small Cell Lung Cancer (SCLC)
Small cell lung cancer (SCLC) is a type of lung cancer that is distinct from other lung cancers due to its clinical and biologic characteristics. It often starts in the bronchi, then quickly grows and spread rapidly (metastasize) to other parts of the body, including the brain, liver, and bone. About 15% of all lung cancer cases are Small cell lung cancer and is slightly more common in men than women. Almost all cases of SCLC are due to cigarette smoking.
Small cell lung cancer is divided into two types, named for the kinds of cells found in cancer and how the cells look when viewed under a microscope:
Small cell carcinoma (oat cell cancer): the cells look like oats under the microscope.
(www.mayoclinic.org/diseases-conditions/lung-cancer)
National Cancer Institute, USA.
Why We Need Research
Research provides hope and saves lives. This is especially true when it comes to lung cancer research. Lung cancer research can help develop better treatments, increasing the survival and quality of life for patients. Research can provide a better and longer future for those diagnosed with lung cancer as well and can also ultimately increase the number of survivors living with the disease.
Simple click showed recent research of LUNG CANCER !!
In the United States, lung cancer is the second most common cancer in both men and women. It’s also the leading cause of death from cancer.
Lung cancer can be serious. However, some people with early stage lung cancer can be successfully treated. This is because tests and treatments for cancer are being studied and improved. If lung cancer is found at an earlier stage when it is small and before it has spread, people have a better chance of living longer.
Current and former smokers are at a higher risk of getting lung cancer as they get older. If they quit, smokers can lower their risk of getting and dying from lung cancer.
Usually symptoms of lung cancer don’t appear until the disease is already at an advanced, non-curable stage. Even if lung cancer does cause symptoms, many people may mistake them for other problems, such as an infection or long-term effects from smoking. This may delay the diagnosis.
Some lung cancers are found early by accident as a result of tests for other medical conditions. For example, lung cancer may be found by tests done for other reasons in people with heart disease, pneumonia, or other lung conditions. A small portion of these people do very well and may be cured of lung cancer.
Screening is the use of tests or exams to find a disease in people who don’t have symptoms. Regular chest x-rays have been studied for lung cancer screening, but they did not help most people live longer. In recent years, a test known as a low-dose CAT scan or CT scan (LDCT) has been studied in people at a higher risk of getting lung cancer. LDCT scans can help find abnormal areas in the lungs that may be cancer. Research has shown that using LDCT scans to screen people at higher risk of lung cancer saved more lives compared to chest x-rays. For higher risk people, getting yearly LDCT scans before symptoms start helps lower the risk of dying from lung cancer.
The National Lung Screening Trial
The National Lung Screening Trial (NLST) was a large clinical trial that looked at using LD CT scan of the chest to screen for lung cancer. CT scans of the chest provide more detailed pictures than chest x-rays and are better at finding small abnormal areas in the lungs. (Both of these tests are discussed in more detail in Exams and tests to look for lung cancer.) Low-dose CT of the chest uses lower amounts of radiation than a standard chest CT and does not require the use of intravenous (IV) contrast dye.
The NLST compared LDCT of the chest to chest x-rays in people at high risk of lung cancer to see if these scans could help lower the risk of dying from lung cancer. The study included more than 50,000 people aged 55 to 74 who were current or former smokers and were in fairly good health. To be in the study, they had to have at least a 30 pack-year history of smoking. A pack-year is the number of cigarette packs smoked each day multiplied by the number of years a person has smoked. Someone who smoked a pack of cigarettes per day for 30 years has a 30 pack-year smoking history, as does someone who smoked 2 packs a day for 15 years. Former smokers could enter the study if they had quit within the past 15 years. The study did not include people if they had a prior history of lung cancer or lung cancer symptoms, if they had part of a lung removed, if they needed to be on oxygen at home to help them breathe, or if they had other serious medical problems.
People in the study got either 3 LDCT scans or 3 chest x-rays, each a year apart, to look for abnormal areas in the lungs that might be cancer. After several years, the study found that people who got LDCT had a 20% lower chance of dying from lung cancer than those who got chest x-rays. They were also 7% less likely to die overall (from any cause) than those who got chest x-rays.
Screening with LDCT was also shown to have some downsides that need to be considered. One drawback of this test is that it also finds a lot of abnormalities that have to be checked out with more tests, but that turn out not to be cancer. (About 1 out of 4 CT scans in the NLST showed such a finding.) This may lead to additional tests such as other CT scans or more invasive tests such as needle biopsies or even surgery to remove a portion of lung in some people. These tests can sometimes lead to complications (like a collapsed lung) or rarely, death, even in people who do not have cancer (or who have very early stage cancer).
LDCTs also expose people to a small amount of radiation with each test. It is less than the dose from a standard CT, but it is more than the dose from a chest x-ray. Some people who are screened may end up needing more CT scans, which means more radiation exposure. When done in tens of thousands of people, this radiation may cause a few people to develop breast, lung, or thyroid cancers later on.
The NLST was a large study, but it left some questions that still need to be answered. For example, it’s not clear if screening with LDCT scans would have the same effect if different people were allowed in the study, such as those who smoke less (or not at all), or people younger than age 55 or older than 74. Also, in the NLST, patients got 3 scans over 2 years. It’s not yet clear what the effect would be if people were screened for longer than 2 years.
These factors, and others, need to be taken into account by people and their doctors who are considering lung cancer risk and the decision to be screened.
American Cancer Society Guidelines for Lung Cancer Screening
The American Cancer Society (ACS) has a lung cancer screening guideline for people with a higher risk of getting lung cancer. The ACS recommends yearly lung cancer screening with LDCT scans for people who are 55 to 74 years old, are in fairly good health, and who also meet the following conditions:
Are current smokers or smokers who have quit in the past 15 years. and
Have at least a 30 pack-year smoking history. (This is the number of years you smoked multiplied by the number of packs of cigarettes per day. For example, someone who smoked 2 packs per day for 15 years [2 x 15 = 30] has 30 pack-years of smoking. A person who smoked 1 pack per day for 30 years [1 x 30 = 30] also has 30 pack-years of smoking.) and
Receive counseling to quit smoking if they are current smokers. and
Have been told by their doctor about the possible benefits, limits, and harms of screening with LDCT scans. and
Have a facility where they can go that has experience in lung cancer screening and treatment.
For Patients
The main benefit of screening is a lower chance of dying of lung cancer, which accounts for many deaths in current and former smokers. Still, it’s important to be aware that, like with any type of screening, not everyone who gets screened will benefit. Screening with LDCT will not find all lung cancers, and not all of the cancers that are found will be found early. Even if a cancer is found by screening, you may still die from lung cancer. Also, LDCT often finds things that turn out not to be cancer, but have to be checked out with more tests to know what they are. You might need more CT scans, or even invasive tests such as a lung biopsy, in which a piece of lung tissue is removed with a needle or during surgery. These tests have risks of their own (see above).
If you are at a higher risk, your doctor can explain your risk and how you fit into the ACS lung cancer screening guideline. Your doctor can also talk with you about what happens during screening and the best places to get the yearly screening test. Lung cancer screening is covered by Medicare and by many private health insurance plans. Your health care team can help you find out if your insurance will provide coverage.
Screening should only be done at facilities that have the right type of CT scanner and that have a lot of experience in LDCT scans for lung cancer screening. The facility should also have a team of specialists that give patients the appropriate care and follow-up if there are abnormal results on the scans. You might not have the right kind of facility nearby, so you may need to travel some distance to be screened.
If you are at higher risk and should be screened, you should get a LDCT every year until you reach the age of 74, as long as you are still in good health.
If you smoke, you should get counseling about stopping. You should be told about your risk of lung cancer and referred to a smoking cessation program. Screening is not a good alternative to stopping smoking. For help quitting, see our Guide to Quitting Smoking or call the American Cancer Society at 1-800-227-2345.
What Does “In Fairly Good Health” Mean?
Screening is meant to find cancer in people who do not have symptoms of the disease. People who already have symptoms that might be caused by lung cancer may need tests such as CT scans to find the underlying cause, which in some cases may be cancer. But this kind of testing is for diagnosis and is not the same as screening. Some of the possible symptoms of lung cancer that kept people out of the NLST were coughing up blood and weight loss without trying.
To get the most benefit from screening, patients need to be in good health. For example, they need to be able to have surgery and other treatments to try to cure lung cancer if it is found. Patients who need home oxygen therapy probably couldn’t withstand having part of a lung removed, and so are not candidates for screening. Patients with other serious medical problems that would shorten their lives or keep them from having surgery might not benefit enough from screening for it to be worth the risks, and so should also not be screened.
Metal implants in the chest (like pacemakers) or back (like rods in the spine) can interfere with x-rays and lead to poor quality CT images of the lungs. People with these types of implants were also kept out of the NLST, and so should not be screened with CT scans for lung cancer according to the ACS guidelines.
If Something Abnormal Is Found Curing Screening
Sometimes screening tests will show something abnormal in the lungs or nearby areas that might be cancer. Most of these abnormal findings will turn out not to be cancer, but more CT scans or other tests will be needed to be sure. Some of these tests are described in Exams and tests that look for lung cancer.
CT scans of the lungs can also sometimes show problems in other organs that just happen to be in the field of view of the scans. Your doctor will discuss any such findings with you if they are found.
If your doctor thinks you might have lung cancer based on the results of a screening test or because of symptoms you are having, he or she will do exams and tests to find out for sure.
Medical History and Physical Exam
Your doctor will ask about your medical history to learn more about any symptoms you are having and possible risk factors. Your doctor will also examine you for signs of lung cancer or other health problems.
If the results of your history and physical exam suggest you might have lung cancer, more tests will be done.
Tests That Might Be Used to Look for Lung Cancer
Sputum Cytology
For this test, a sample of mucus you cough up from the lungs (sputum) is looked at under a microscope to see if it contains cancer cells. The best way to do this is to get early morning samples from you 3 days in a row.
Chest X-Ray
If you have symptoms that might be due to lung cancer, this is often the first test your doctor will do. Plain x-rays of your chest can be done at imaging centers, hospitals, and even in some doctors’ offices. If something suspicious is seen, your doctor may order more tests.
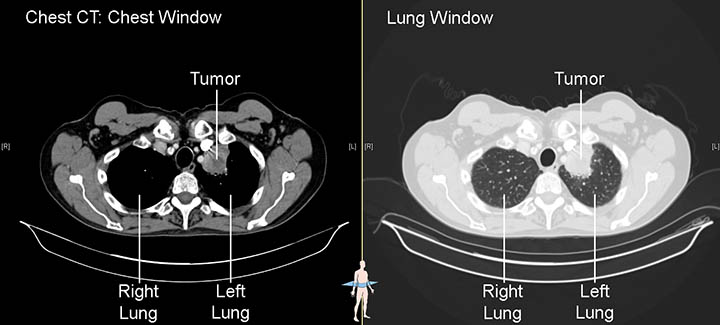
Computed Tomography(CT) Scan
A CT scan uses x-rays to make detailed cross-sectional images of your body. Instead of taking one picture, like a regular x-ray, a CT scanner takes many pictures as it rotates around you while you lie on a table. A computer then combines these pictures into images of slices of the part of your body being studied.
CT scans are more likely to show lung tumors than routine chest x-rays. They can also show the size, shape, and position of any lung tumors and can help find enlarged lymph nodes that might contain cancer that has spread from the lung.
Further Tests If You Have an Abnormal Screening Test Result
When a low-dose CT scan of the chest is done for lung cancer screening, it’s common to find small, abnormal areas (called nodules or masses) in the lungs, especially in current or former smokers. Most lung nodules seen on CT scans are not cancer. They are more often the result of old infections, scar tissue, or other causes. But tests are often needed to be sure a nodule is not cancer.
Most often the next step is to get a repeat CT scan to see if the nodule is growing over time. The time between scans might range anywhere from about a month to a year, depending on how likely your doctor thinks it is that the nodule could be cancer. This is based on the size, shape, and location of the nodule, as well as whether it appears to be solid or filled with fluid. If the nodule is larger, your doctor might also want to get another type of imaging test called a positron emission tomography (PET) scan, which can often help tell if it is cancer.
If the second scan shows that the nodule has grown, or if the nodule has other concerning features, your doctor will want to get a sample of it to check it for cancer cells. This is called a biopsy. This can be done in different ways:
The doctor might pass a long, thin tube (called a bronchoscope) down your throat and into the airways of your lung to reach the nodule. A small, hollow needle on the end of the bronchoscope can be used to get a sample of the nodule.
If the nodule is in the outer part of the lung, the doctor might pass a thin, hollow needle through the skin of the chest wall and into the nodule to get a biopsy sample.
If there is a higher chance that the nodule is cancer (or if the nodule can’t be biopsied with a needle), surgery might be done to remove the nodule and some surrounding lung tissue. Sometimes larger parts of the lung might be removed as well.
Further Tests If You Have Possible Signs or Symptoms of Lung Cancer
If your doctor is concerned you might have lung cancer because of signs or symptoms you are having, a chest x-ray or chest CT scan is likely to be the next step. Other tests that might be done include having you cough up sputum (phlegm) to have it looked at for cancer cells, or having a bronchoscopy, where the doctor puts a long, thin tube down your throat and into your lungs to look for anything abnormal.
If any of these tests are suspicious for cancer, further tests such as a biopsy or even surgery will likely be needed to get samples from any tumors.
"The scary thing about lung cancer is that it can go so long without being symptomatic and that is what makes early detection so important. I was feeling great, but little did I know this disease was growing inside of me." —Ashley M., LUNG FORCE Hero
Nearly a quarter of a million American women and men will be diagnosed with lung cancer this year. Getting a diagnosis when lung cancer is in its early stages and easier to treat is crucial. It can help save lives.
Right now, the best way to detect lung cancer early is through lung cancer screening for high-risk individuals. But for too many people, lung cancer is found by chance. For example:
Thankfully, for Heather, Zelita and Ashley, their lung cancer was diagnosed early and treatment plans were put in place.
New methods of early detection are on the horizon. Three major organizations fighting lung cancer are joining forces to form a lung cancer "Interception Dream Team" to investigate cancer interception—a promising new approach to cancer prevention and treatment. Instead of identifying cancer after it's developed, the Dream Team will investigate a way to stop lung cancer before it even begins.
Screening and potential innovative methods of early detection along with improving treatment options bring new hope for lung cancer patients. That's why the American Lung Association's LUNG FORCE initiative focuses on uniting women and our nation in the effort to defeat lung cancer. Awareness is the critical first step toward saving lives. Awareness is not just understanding what lung cancer is, but also knowing lung cancer risk factors and talking to your doctor about your risks and screening options. And, sharing lung cancer experiences can help bring awareness to others and encourage them to be proactive about their lung health. All of these things are important to finding lung cancer early and getting a treatment plan in place; which gives patients a greater chance of survival. In fact, if lung cancer is caught before it spreads, the likelihood of survival more than triples.
"I am thankful to be alive and stronger each day. Get your check-ups; visit your doctors routinely; and know your close family's medical history." —Zelita W., LUNG FORCE Hero
This Lung Cancer Awareness Month, you can help. If lung cancer has touched your life, #ShareYourVoice to give others courage, help us raise awareness about the disease and the importance of early detection by sharing your story at LUNGFORCE.org.
Lung Cancer Stages
Staging uses the TNM system:
T (tumor): size of the original tumor.
N (node): present in the lymph nodes.
M (metastasis): spread to other parts of the body.
Small Cell Lung Cancer (SCLC) Staging
Limited stage: The cancer is found in one lung, sometimes including nearby lymph nodes.
Extensive stage: Cancer has spread to the other lung, the fluid around the lung (the pleura) or to other organs in the body.
Non-Small Cell Lung Cancer (NSCLC) Staging
Occult-stage: Cancer cells are found in a body fluid such as saliva but no tumor can be found in the lung.
Stage 0: Very small size and has not spread into deeper lung tissues or outside the lungs (carcinoma in situ).
Stage I: Shown in the underlying lung tissues, but not lymph nodes.
Stage II: Spread to nearby lymph nodes or into the chest wall.
Stage III: Continuing to spread from the lungs to the lymph nodes or to nearby organs.
Stage IV: Spread, beyond the lungs into other areas of the body. About 40 percent of patients diagnosed with lung cancer when they are in stage IV.
www.cancercenter.com
www.covenanthealth.com
Diagnosing Lung Cancer
Chest X-Ray
Chest x-ray is often the first test your doctor will do to look for any abnormal areas in the lungs.
Computed Tomography (CT) scan
CT scanner takes many pictures as it rotates around you while you lie on a table to create a 3D picture of the lungs.
Positron Emission Tomography (PET) Scan
PET Scan is a medical imaging technique that uses a radioactive tracer to pinpoint differences in lung tissues on the molecular level.
Endobronchial Ultrasound (EBUS)
EBUS is a less invasive bronchoscopic procedure used to evaluate and sample cancerous cells in the chest. In most cases, EBUS is performed as an alternative to a mediastinoscopy, a surgical procedure used to collect samples in the chest while the patient is under general anesthesia.
Computed Tomography (CT) Angiogram
CT angiography uses a CT scanner to produce detailed images of both blood vessels and tissues in various parts of the body. An iodine-rich contrast material (dye) is usually injected through a small catheter placed in a vein of the arm.
Biopsy
Lung biopsy procedure, the doctor removes a small piece of tissue or fluid from the chest so it can be examined under a microscope to check for cancer cells.
Bronchoscopy
Bronchoscopy is a procedure that looks inside the lung airways. It involves inserting a bronchoscope tube, with its light and a small camera, through your nose or mouth, down your throat into your trachea, or windpipe, and to the bronchi and bronchioles of your lungs.
Testing for genetic mutations
Genetic testing is a type of medical test that identifies changes in chromosomes, genes, or proteins. The results of a genetic test can confirm or rule out a suspected genetic condition or help determine a person’s chance of developing or passing on a genetic disorder. More than 1,000 genetic tests are currently in use, and more are being developed.
Several methods can be used for genetic testing:
Molecular genetic tests (or gene tests) study single genes or short lengths of DNA to identify variations or mutations that lead to a genetic disorder.
Chromosomal genetic tests analyze whole chromosomes or long lengths of DNA to see if there are large genetic changes, such as an extra copy of a chromosome, that cause a genetic condition.
Biochemical genetic tests study the amount or activity level of proteins; abnormalities in either can indicate changes to the DNA that result in a genetic disorder.
Clinical trials are research studies that involve people. Through clinical trials, doctors find new ways to improve treatments and the quality of life for people with disease.
Researchers design cancer clinical trials to test new ways to:
Treat cancer
Find and diagnose cancer
Prevent cancer
Manage symptoms of cancer and side effects from its treatment
Clinical trials are the final step in a long process that begins with research in a lab. Before any new treatment is used with people in clinical trials, researchers work for many years to understand its effects on cancer cells in the lab and in animals. They also try to figure out the side effects it may cause.
Any time you or a loved one needs treatment for cancer, clinical trials are an option to think about. Trials are available for all stages of cancer. It is a myth that they are only for people who have advanced cancer that is not responding to treatment. To look for trials, see Find NCI-Supported Clinical Trials.
Every trial has a person in charge, usually a doctor, who is called the principal investigator. The principal investigator prepares a plan for the trial, called a protocol. The protocol explains what will be done during the trial. It also contains information that helps the doctor decide if this treatment is right for you. The protocol includes information about:
The reason for doing the trial
Who can join the trial (called “eligibility criteria”)
How many people are needed for the trial
Any drugs or other treatments that will be given, how they will be given, the dose, and how often
What medical tests will be done and how often
What types of information will be collected about the people taking part
Why Are Clinical Trials Important?
Today, people are living longer lives from successful cancer treatments that are the results of past clinical trials. Through clinical trials, doctors determine whether new treatments are safe and effective and work better than current treatments. Clinical trials also help us find new ways to prevent and detect cancer. And they help us improve the quality of life for people during and after treatment. When you take part in a clinical trial, you add to our knowledge about cancer and help improve cancer care for future patients. Clinical trials are the key to making progress against cancer.